1570596441 by Unknown
Author:Unknown
Language: eng
Format: epub
290 Nuclear Medicine Figure 4. A 12 year old girl who presented with papillary carcinoma with lymph node and diffuse pulmonary metastases. Her presenting pO2 was 50. Several RAI treatments were given along with steroids to minimize pulmonary fibrosis. This ablated the lymph node but did not change the lung uptake. She died of cardiopulmonary failure 10 years later. including the United States and Canada, there is no longer a rigid requirement to admit patients for large dose therapies. Most thyroid cancer patients do not require supportive hospital care. If they are admitted, it is because they do not have the domestic facilities necessary for self- sequestration at home, that they have come for treatment from a distance or with public transportation, or that they are considered to be unlikely to follow instructions. If these patients were treated as out-patients, they would constitute a source of radiation exposure to members of the public or to juvenile or pregnant family members. Thus, some patients are still best treated in hospital. For others, out-
Radionuclide therapy of Thyroid Disorders 291 Figure 5. A 62 year old woman who presented with a pathological fracture secondary to metastatic follicular carcinoma. Her hemoglobin was 80g/ L and platelets <100x109/L With RAI therapy her disease regressed and bone marrow function normalized but the bone metastases were never ablated. She remained active for most of the next 14 years, requiring repeated RAI treatments and occasional external beam treatments when she developed non-iodi ne-avid metastases. patient treatment is both safe and preferable in terms of availability of the emotional support from families. The requirement for safe home treatment is that family and other close associates of the patient do not receive more dosage than is permitted by the local nuclear safety regulations. The instructions for at home behaviour will be similar to those given to patients treated for benign disease except that they will take account of the small to absent organified component. As a result, iodine is much more rapidly eliminated from the body. Patients who are totally athyrotic and have no tumor uptake may be nearly clear of radioactivity by 2-3 days. Those with remnants and a significant uptake will need to remain isolated for a longer time. The patient can be given a behavioural
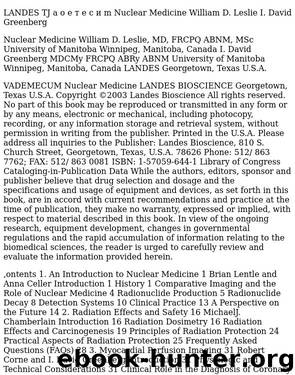
292 Nuclear Medicine Figure 6. A 26 year old woman with papillary carcinoma of thyroid. Her tumor does not secrete Tg. The first post-surgical scan showed bilateral positive nodes in her neck and the follow-up scan showed clearing after one RAI treatment. She then developed recurrent neck node disease. After a bilateral neck dissection she had a negative post-therapy RAI scan. However the FDG PET scan showed multiple nodes in the upper mediastinum, a finding confirmed by a subsequent CT scan. The image is a coronal section. The margins of the neck are defined by FDG uptake into the sternocleidomastoid muscles and the positive nodes are located centrally.
Radionuclide therapy of Thyroid Disorders 293 Figure 7. A woman in her 60s who has pulmonary and neck metastases from a papillary carcinoma that does not take up iodine as in (a).
Download
This site does not store any files on its server. We only index and link to content provided by other sites. Please contact the content providers to delete copyright contents if any and email us, we'll remove relevant links or contents immediately.
Becoming Supernatural by Dr. Joe Dispenza(8277)
Crystal Healing for Women by Mariah K. Lyons(7965)
The Witchcraft of Salem Village by Shirley Jackson(7338)
Inner Engineering: A Yogi's Guide to Joy by Sadhguru(6836)
The Four Agreements by Don Miguel Ruiz(6835)
The Power of Now: A Guide to Spiritual Enlightenment by Eckhart Tolle(5854)
Secrets of Antigravity Propulsion: Tesla, UFOs, and Classified Aerospace Technology by Ph.D. Paul A. Laviolette(5412)
The Wisdom of Sundays by Oprah Winfrey(5206)
Room 212 by Kate Stewart(5184)
Pale Blue Dot by Carl Sagan(5081)
Fear by Osho(4782)
The David Icke Guide to the Global Conspiracy (and how to end it) by David Icke(4771)
Rising Strong by Brene Brown(4512)
Animal Frequency by Melissa Alvarez(4511)
How to Change Your Mind by Michael Pollan(4403)
Sigil Witchery by Laura Tempest Zakroff(4297)
Man and His Symbols by Carl Gustav Jung(4196)
The Art of Happiness by The Dalai Lama(4169)
Real Magic by Dean Radin PhD(4168)
